
While likely more than 80,000 U.S. residents filled a prescription for Truvada (tenofovir/emtricitabine) as pre-exposure prophylaxis (PrEP) by the end of 2015, its use among young people, minorities, women and people in many parts of the South, where HIV transmissions are particularly high, lags behind, aidsmap reports. Gilead Sciences released an updated of PrEP use in the United States at the 21st International AIDS Conference in Durban, South Africa (AIDS 2016).
Gilead researchers based their prescription estimates on available data from 80 percent of U.S. retail pharmacies that dispensed Truvada between January 2012 and December 2015. They used an algorithm to exclude prescriptions written for non-PrEP purposes (there is no specific prescription code for Truvada’s use as PrEP), including HIV treatment, HIV post-exposure prophylaxis (PEP) and hepatitis B virus (HBV) treatment.
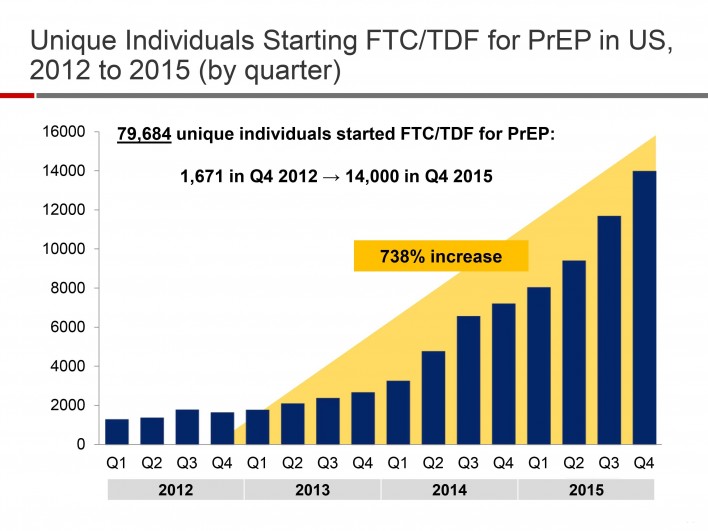
By the end of the study period, 79,684 people filled at least one PrEP prescription. Considering that researchers did not have access to the entirety of U.S. pharmacy data, presumably the actual number of prescriptions written during that time was greater. Between the fourth quarter of 2012 and the same quarter of 2015, new PrEP prescriptions rose 738 percent, from 1,671 to 14,000.
What data was available about the race of those receiving PrEP aligned with previous findings: that the population is largely white. This raises the issue of the potential breadth of PrEP’s impact on HIV infection rates, considering how disproportionately the virus impacts African Americans in particular. If PrEP is predominantly used by white men who have sex with men (MSM) and succeeds in driving down their rate of annual HIV infections at a faster rate (the figures have long been falling), this may effectively widen existing racial disparities in HIV incidence among MSM as a whole.
Divided by sex, new PrEP prescriptions were not far from even in 2012: 3,470, or 56 percent of the 6,210 prescriptions written for men. The number of prescriptions for women rose from 2,740 in 2012 to 7,313 in 2015 but did not rise at a rate nearly as quickly as prescriptions for men. In 2015, 35,232, or 82 percent of the 42,545 new prescriptions were for men.
Overall, the average age of people starting PrEP during the study period was 36.2, or 33.2 among women and 37.1 among men. Twenty-eight percent of the women were younger than 25, as were 11 percent of the men. The average age of the women starting PrEP in 2012 and 2015 was a respective 34 and 33.4. For men, the corresponding ages were 39.2 and 36.7.
Five major states accounted for half of those starting PrEP, including California (16.7 percent), New York (15.9 percent), Texas (6.8 percent), Florida (5.7 percent) and Illinois (5.4 percent). States accounting for more than 2 percent of first-time PrEP prescriptions included Massachusetts (5.1 percent), Pennsylvania (4.7 percent), Georgia (3.7 percent), Washington (3.5 percent), Washington, DC (3.3 percent), New Jersey (2.5 percent), Minnesota (2.5 percent) and Ohio (2.1 percent).
Massachusetts had the highest percentage of its state population starting PrEP (4,950 people), followed by New York (12,588), Illinois (4,302), Florida (5,675), California (10,437), New Jersey (2,301), Pennsylvania (2,878), Georgia (2,230), Texas (5,120) and Ohio (2,156).
Broken down by city, 39 to 55 percent of individuals’ first PrEP prescriptions were written in 2015. The largest numbers were in New York (2,936), San Francisco (1,094), Chicago (1,001), Washington, DC (840), Los Angeles (660), Seattle (574), Boston (548), Atlanta (524) and Philadelphia (500).
The Gilead report concluded that barriers to PrEP use should be addressed in demographics at high risk for HIV, including women, those younger than 25 and states with high HIV rates.
To read the aidsmap article, click here.
Courtesy of Gilead

Courtesy of Gilead

Courtesy of Gilead




Comments
Comments